The Solution- The Dashboard
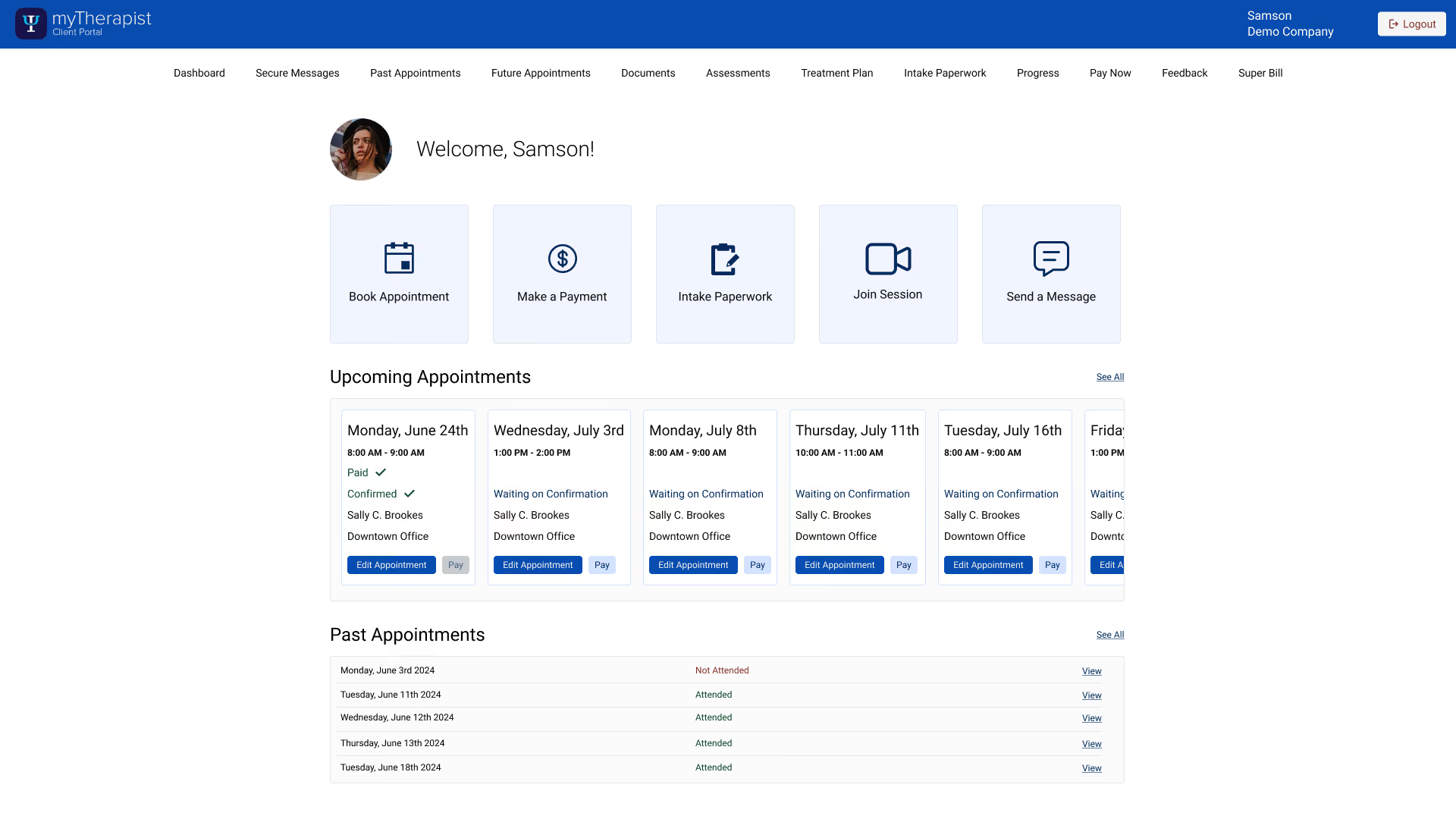
One home screen, three actions, no hunting
The redesign's backbone is a single dashboard that puts a patient's key actions one tap away: book an appointment, pay, and complete intake paperwork, all from one place instead of scattered across pages a patient had to learn. It opens on what matters daily — the next appointment and a clear balance with one way to pay it. Past appointments show their details cleanly, and payment is reframed around the balance, so patients can pay in full or in part without reasoning about session costs and insurance math that was never theirs to untangle.
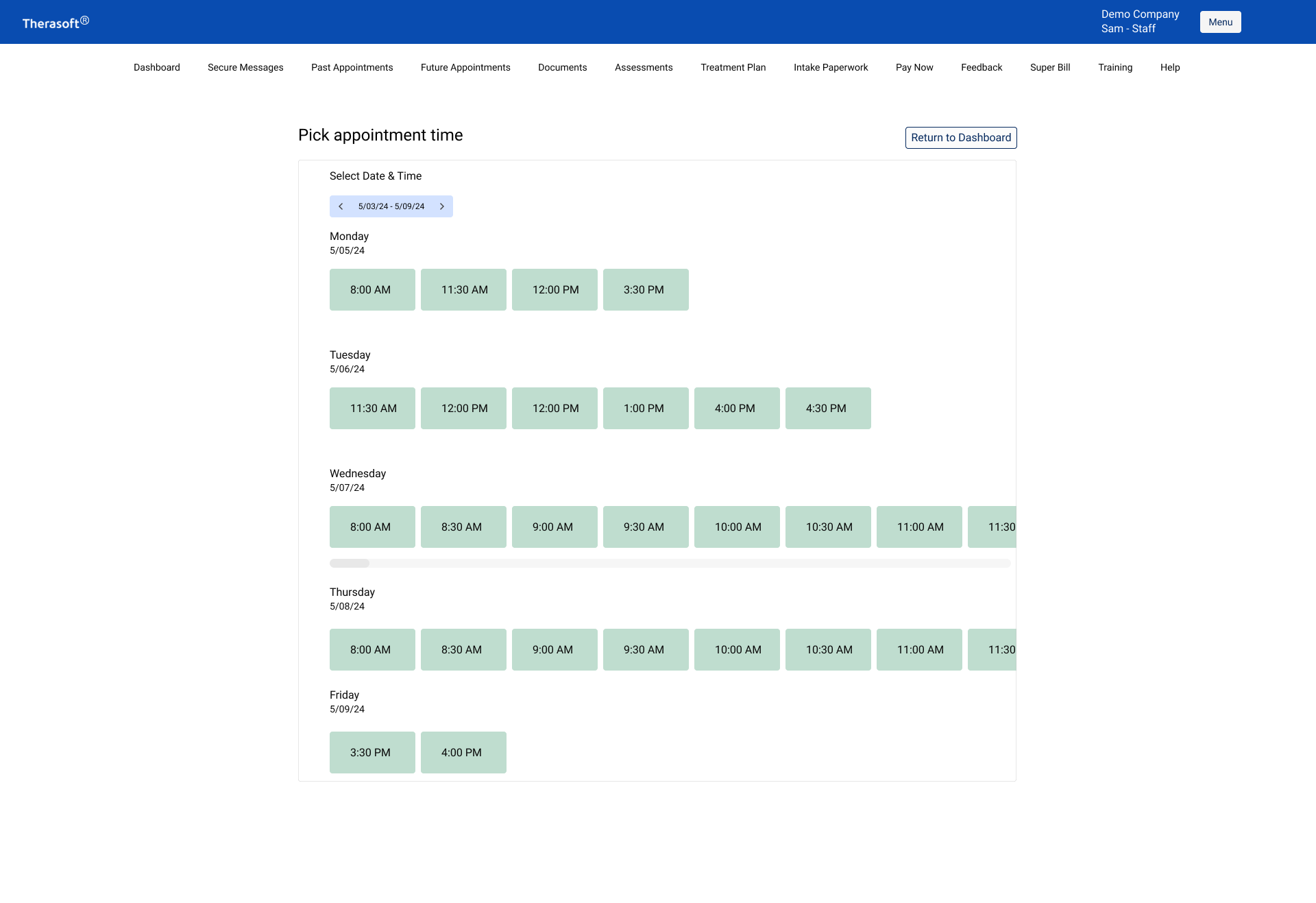
"Show what's open, never reveal what's taken"
- Design principle behind the booking flow